The 1994 genocide against the Tutsi in Rwanda killed more than 1 million people in just 100 days and decimated the country's infrastructure, including its health system. More than 94% of the survivors in Rwanda witnessed the murder of a family member or demolition of their property. Decades later, many still struggle to cope with their memories of war and suffer from mental health disorders. The most prevalent mental disorders are posttraumatic stress disorder (PTSD), depression, and panic disorder.
Adult survivors are not the only ones enduring the long-lasting effects of the genocide; the symptoms of PTSD also manifest in many of the survivors' children through epigenetics, chemical modifications to the DNA code often influenced by the environment or stress. Despite that adversity, Rwanda has demonstrated remarkable resilience in rebuilding its economy and health system, particularly in addressing its mental health crisis. Its success in overcoming the collective trauma caused by the genocide can be attributed to a variety of factors, including the government's pursuit of strategic partnerships and innovative solutions to navigating mental health care.
Community-Based Sociotherapy
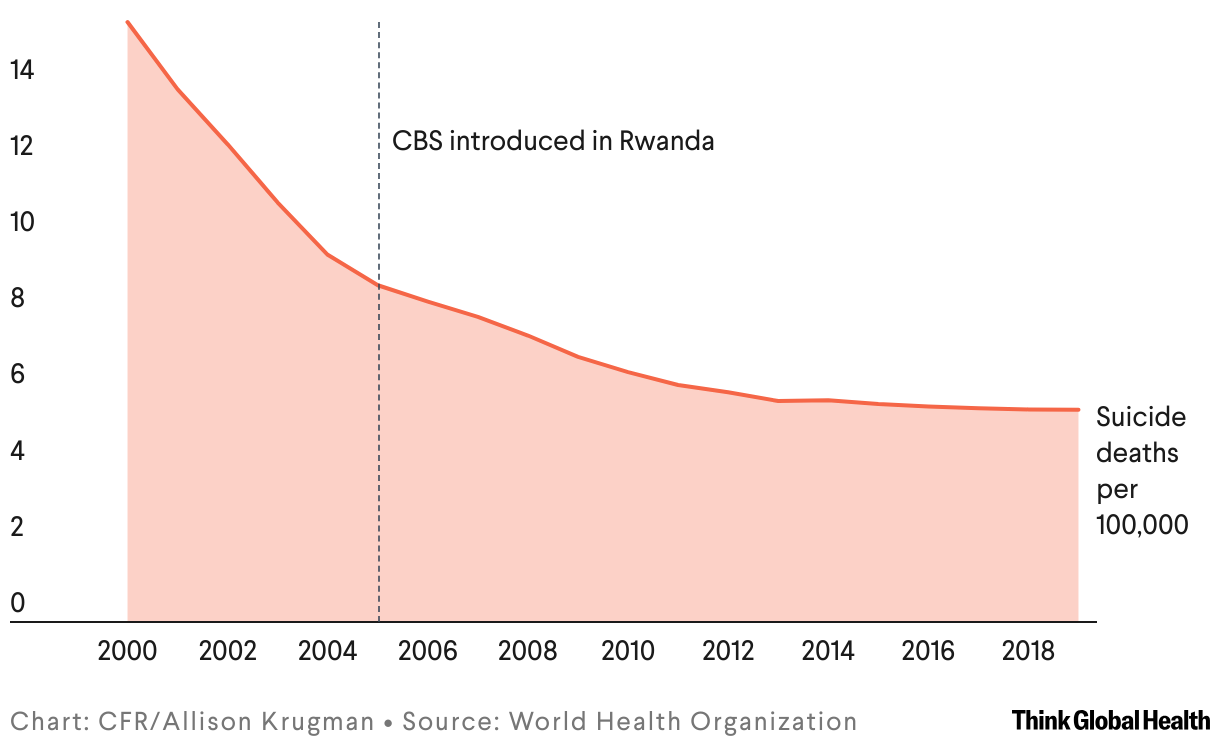
To navigate the aftermath of the genocide, the ministry of health (MoH) and partners launched Mvura Nkuvure, a community-based sociotherapy (CBS) model whose name translates to "Heal me, I heal you," to facilitate healing and peacebuilding for survivors. Since its adoption, participants have reported an increased sense of redress, social cohesiveness, and decreased conflicts between survivors and perpetrators. Results from studies on CBS's impact indicate that the model had positive effects on participants' mental health and overall well-being. This is also justified by the gradual drop in crude suicide mortality in Rwanda since the launch of CBS.
The Six Phases of Community-Based Psychotherapy (CBS)
CBS guides participants through six consecutive phases, each with a specific theme
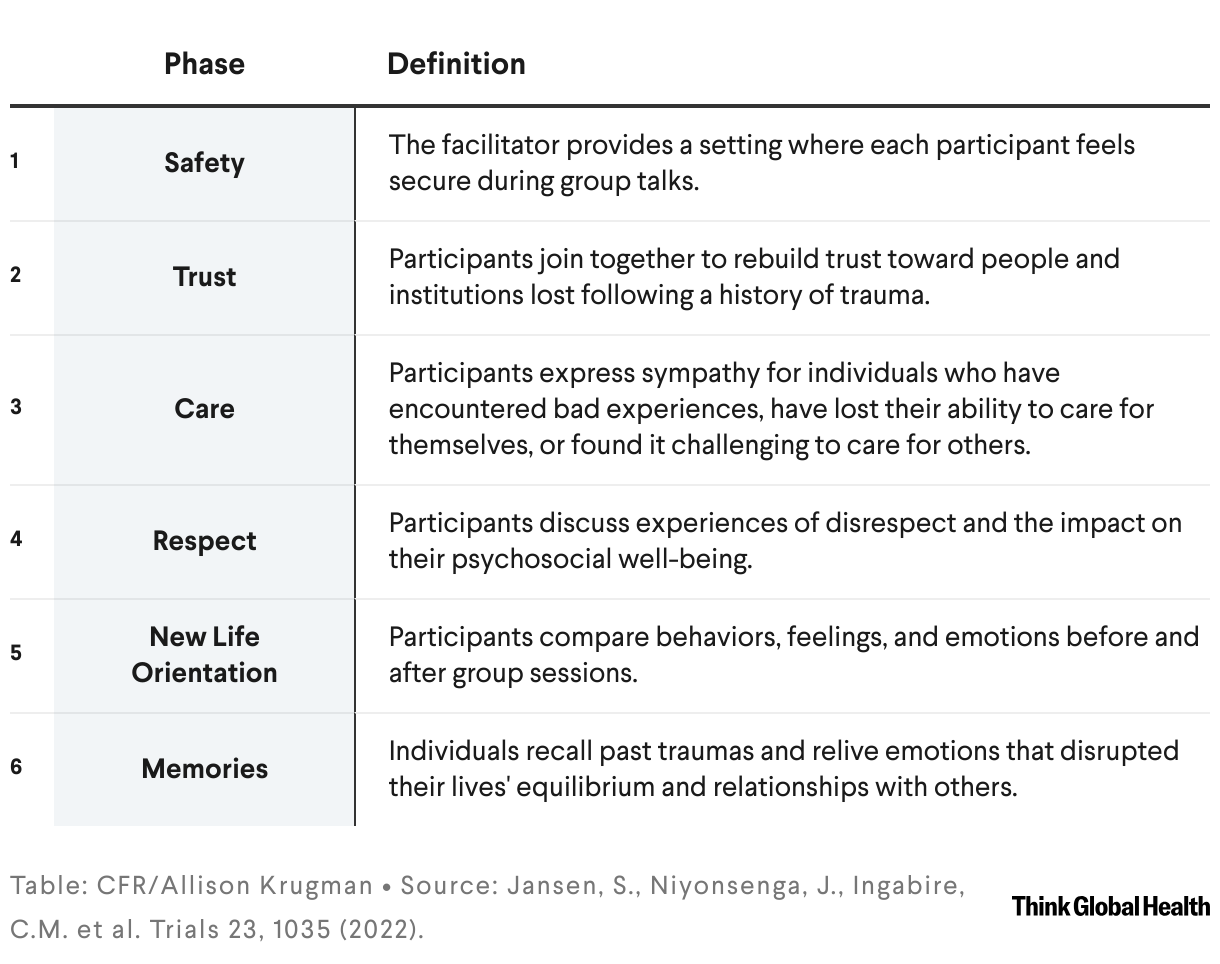
Part of the model's success can be attributed to how it complements efforts by the government to reconcile Tutsi and Hutu Rwandans through therapy. The CBS model consists of safety, trust, care, respect, new life orientation, and memories.
Despite the progress brought forward by the implementation of CBS, the country was still struggling to meet the demand for mental health services by early 2010s due to a shortage of mental health providers. To address this, the Ministry of Health decided to integrate mental health services into primary care. That involved building capacity for primary care nurses and community health workers (CHWs) and improving the quality of mental health services through continuous mentorship, supervision, and feedback.
Suicide Deaths Drop in Rwanda
Mental health and well-being in Rwanda have improved in the years following the 1994 genocide, aided by community-based sociotherapy (CBS)
The training focused on teaching CHWs how to distribute educational materials and identifying mental health disorders. Although this integration increased the mental health provider-to-patient ratio from almost less than 1 in early 2000s to 3.98 per 100,000 in 2020, it has not yet been implemented across all parts of the country due to limited resources needed for a national rollout.
A Tailored Justice System
After the genocide, the Government of National Unity sought to normalize relations between Hutu and Tutsi Rwandans. To accomplish this, they established Gacaca courts, a new judicial system to provide restorative justice for survivors and create space for reconciliation between the survivors and perpetrators. It emphasized accountability and involved partial or absolute commutation of prison sentences in turn for community service for those who confessed their crimes.
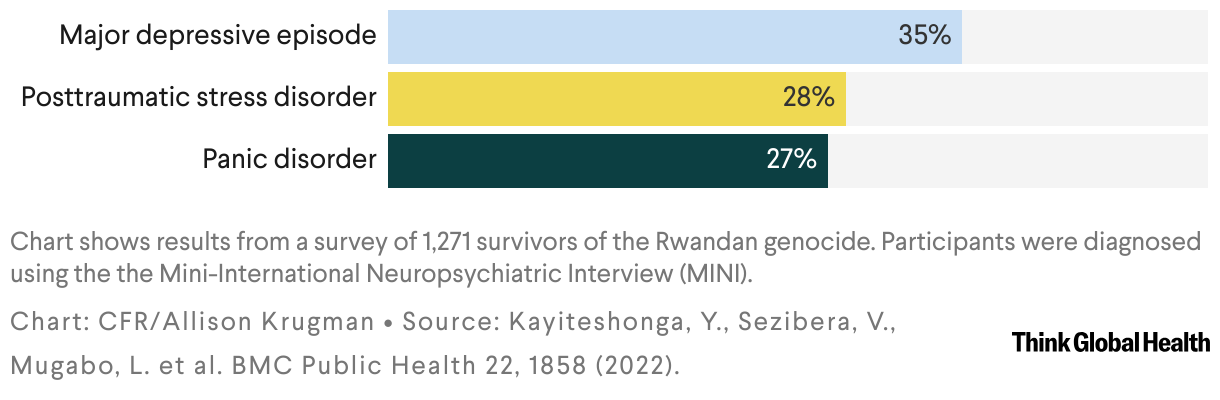
Mental Disorders Persist in Rwandan Genocide Survivors
A survey conducted in 2018 found a high prevalence of major mental disorders among participants
That process was locally known as ibihano nsimbura gifungo, meaning punishments in substitute for incarceration. It also incentivized more perpetrators to confess in exchange for parole. The Gacaca courts helped process trials that would have otherwise taken more than 100 years to see through. As a result, more than 1.2 million cases were tried in more than 12,000 Gacaca courts.
Universal Health Coverage
By 2000, Rwanda had achieved substantial progress in restoring peace and stability within its borders, enabling the government to invest in projects that raised the quality of life among its citizens. One of the major achievements was the community-based health insurance scheme, Mutuelle de Santé, which provides universal health coverage (UHC) for conditions, including mental health, for just $2 per person per year. Since Mutuelle de Santé was fully implemented in 2006, the country's overall life expectancy at birth has risen from 56 to 70.
Challenges Beyond the Triumphs
Despite investments in mental health, challenges in use of the services persist. One study from 2022 demonstrates that uptake for mental health care remains low (5.3%) despite the rise in the awareness of mental health services (61.7%). Although awareness is a crucial first step in the mental health-care cycle, it is not enough to incentivize uptake of health services. Data shows that many Rwandans forgo treatment because they have a limited understanding of mental health, a lack of money, and no transportation.
Despite investments in mental health, challenges in use of the services persist
Although scaling up the integration of mental health into primary care has the potential to address the issue of limited resources, overcoming cultural barriers and fallacies around mental health care of might require a different strategy altogether. Policymakers and implementers should consider enacting a classroom-based mental health curriculum and integrating it into the existing academic systems as a sustainable way to increase mental health literacy for students. As part of the implementation, teachers across primary and secondary should be provided with training, mentorship, audit, and feedback as well as supervision. Evidence from Tanzania and Canada shows that school-based mental health literacy interventions effectively improve mental health awareness and reduce stigma. In both Tanzania and Canada, this intervention has proven to promote mental health, decrease stigma, and enhance self-care practices among participants.