Rwanda is battling its first outbreak of Marburg virus, a severe and often fatal disease. Discovered less than two weeks ago, the outbreak is already the third largest on record, accounting for 58 confirmed cases and 13 deaths as of October 10.
Despite the ostensible delay in detection, once the outbreak was recognized and declared on September 27, 2024, the Rwandan Ministry of Health launched an ambitious response to contain the spread—scaling up clinical care resources, dramatically expanding testing, and reaching out to global partners for international expertise and access to experimental medical countermeasures.
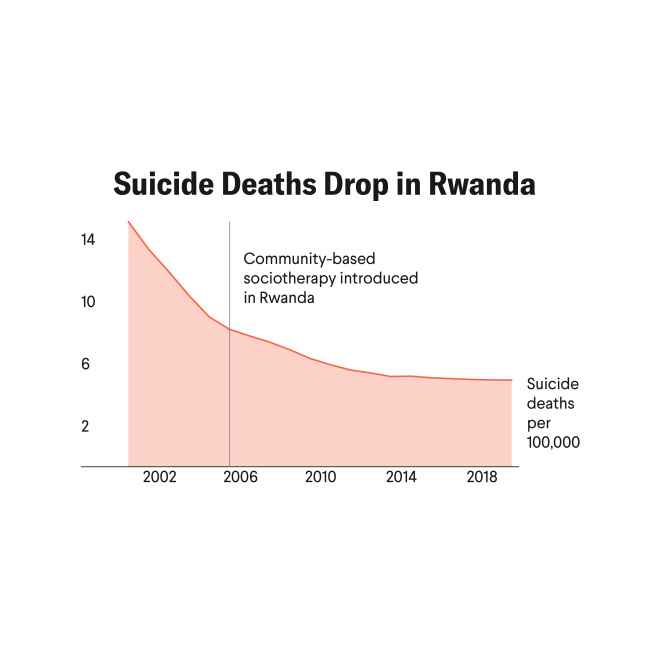
Rwanda's response to Marburg has been helped by its health system, which has rebuilt from the ashes of the genocide three decades ago to become one of the strongest in the region. Even with this infrastructure, the emergency has posed a significant challenge and important lessons are emerging about preparing for and responding to future outbreaks and global health security.
Having worked in the field response to multiple outbreaks, including as physician and a country-level epidemiologist in Guinea during Ebola in 2014, I know the next few weeks could be even harder as they work to get it under control and prevent further spread, especially among their own health-care workforce and to other countries.
Yet we've already seen promising signs.
Marburg, Briefly Explained
Marburg belongs to the same virus family as Ebola (filoviruses), and the approach to containing each disease is similar. Like Ebola, Marburg spreads from human to human via infected body fluid and has a similar incubation period (2–21 days). Both diseases can cause fever, headache, diarrhea, and severe bleeding. Fatality rates up to 88% have been reported for Marburg, but good clinical care can lower that figure.
The Marburg virus was first discovered in 1967 when laboratory workers in Marburg and Frankfurt-am-Main, West Germany, and Belgrade, Serbia (then Yugoslavia), simultaneously fell ill after handing African green monkeys imported from Uganda.
In total, 18 Marburg outbreaks have been reported; their frequency appears to be increasing, with five outbreaks in the last three years alone.
Rwanda's Health System, Clinical Care Needs, and Early Promise
Building on expertise learned during the COVID pandemic, Rwanda's contact tracing for Marburg was quickly put in place in an effort to understand the different chains of transmission. This labor-intensive work requires epidemiologists to compile exhaustive lists of any people who could have been in contact with a confirmed case. Each identified contact is then followed for 21 days to record symptoms, monitor temperature, and refer anyone for testing. Rwanda has reported that it is following more than 400 contacts.
Rwanda's response to Marburg has been helped by its health system, which has rebuilt from the ashes of the genocide three decades ago
The current Marburg outbreak in Rwanda is in many ways typical for filovirus outbreaks. As is often the case, recognition and confirmation of the diagnosis was delayed. Epidemiologic analysis has tied the index case back to September 8, nearly three weeks before the outbreak was declared late in the month. No case of Marburg had ever been reported in Rwanda, which likely delayed the initial diagnosis. Similarly, the index case tested positive for malaria, ostensibly providing an explanation for his symptoms and preventing any further exploration of his death.
More than 80% of the initial Marburg cases were in health-care workers, a common finding in the early days of filovirus outbreaks, when disease spread takes place within health structures. Providers often come in close contact with patients who present for care at the most infectious phase of their illness.
In developing clinical capacity for Marburg outbreaks, two goals are critical: reduce the risk of infection for providers while providing high-quality clinical care to patients. Both are resource and labor intensive, requiring a sufficient supply of personal protective equipment and the implementation of strict protocols to reduce exposure risk.
No vaccines or therapeutics for Marburg are currently approved, but experimental treatments—including monoclonal antibodies and an antiviral drug—have already reached Rwanda and are being used in patient care.
Otherwise, the mainstay of treatment is early and intensive supportive care, which can help lower mortality. This requires medical providers to perform frequent assessment of vital signs and address any abnormalities, appropriately replace fluid losses, monitor laboratory results (including kidney and liver function), and perform potentially more clinically demanding and higher risk interventions such as renal dialysis or intubation. This also requires vast quantities of personal protective equipment and strict adherence to protocols created for safely using it, particularly for properly removing it when the risk of exposure is highest.
A remarkable achievement is the arrival of an experimental Marburg vaccine just days after the outbreak was reported. More than 700 doses were provided by the Sabin Vaccine Institute, a nonprofit organization promoting global vaccine development, and another 1,000 doses will reportedly arrive soon in the country. These vaccines were developed with significant financial and research backing from the Administration for Strategic Preparedness and Response (ASPR) and the National Institutes of Health (NIH), highlighting the importance of U.S. contributions to supporting global health response.

The swift deployment of vaccines in Rwanda contrasts sharply with that for previous filovirus outbreaks, when complicated paperwork and formal bureaucracy often delayed arrival of vaccines and other medical countermeasures until after the period they could be used in a trial, most recently in the 2022 Ebola Sudan outbreak in Uganda.
Yet these vaccine doses arrived in Rwanda within a week of the request and were already being administered to frontline providers the day they arrived.
International Risk: Avoiding Past Missteps
Outside the confines of its hospitals, Rwanda will face different challenges in containing this outbreak. Cases were initially reported from seven of Rwanda's 30 districts, with most concentrated in and around the capital city, Kigali. During the 2014–2016 West Africa Ebola outbreak, transmission to capital cities led to a dramatic rise in case counts given the greater level of potential exposure.
Similarly, Rwanda's capital is a global travel hub and booming tourist destination, with more then 1.4 million arrivals last year and direct connections to London, Paris, and many other country destinations. As a result, Rwanda has put in place guidelines and issued travel advisories, as has the Centers for Disease Control and Prevention (CDC) in an effort to "inform clinicians and health departments" about the outbreak. On October 7, the U.S. Department of Health and Human Services issued a press release outlining a plan to begin, next week, public health entry screening of travelers entering the United States who have been in Rwanda in the past 21 days to "reduce the risk of importation of Marburg cases."
Outside the confines of its hospitals, Rwanda will face different challenges in containing this outbreak
The following day, the Africa CDC released a statement criticizing any travel bans or restrictions, arguing these measures are "inconsistent with international health guidelines and risk undermining public health responses, deepening economic challenges, and reigniting the inequities and mistrust that surfaced during the COVID-19 pandemic."
Potentially more concerning is the risk of international spread to Rwanda's neighbors, notably in Burundi and Democratic Republic of Congo where instability, weak health infrastructure, and the ongoing mpox outbreak would hamper the ability to launch the scale of response needed to contain Marburg.
The Give and Take of Information Sharing
A week into the outbreak, global experts outside the country expressed frustration with a perceived deficiency of important data. Virologists wanted more genomic information, epidemiologists wanted greater clarity on the contact tracing, and health-care providers wanted more clinical data.
Given my field experience with the 2014 Ebola response, I understand how difficult and time consuming it is to conduct this disease detective work, especially while trying to manage requests from an influx of international experts, setting up auxiliary structures for isolation and clinical care, ramping up testing capacity, and overseeing a growing number of meetings and interview requests. This data gathering and reporting is sometimes a challenge even in countries with excellent technical capacity, as evidenced by the current response to H5N1 bird flu outbreak in the United States.
During the COVID-19 pandemic, society became accustomed to nearly instantaneous updates on the number of new cases or hospital capacity. These are important metrics to help guide response but take significant time and effort to step up, especially in the early days of any new outbreak. International requests come as leaders haggle over the pandemic agreement—and to what degree low- or middle-income countries should receive medical products in return for sharing information on emerging outbreaks.
African nations are increasingly seeking to assert their independence on public health. They have not forgotten the inequitable distribution of COVID-19 vaccines that put many African countries last in the global queue. The Africa Union recently set a goal to produce 60% of the vaccines needed on the continent by 2040, up from less than 1% today. To that end, Rwanda recently opened a mRNA vaccine manufacturing facility in Kigali.
They have also not forgotten the punitive travel bans put in place after scientists in South Africa first discovered the COVID-19 variant omicron in November 2021. The bans targeted seven southern African countries, lasted more than a month, hobbled the region's much-needed tourism industry, and ultimately did little to prevent the new variant's spread. If the global community expected greater transparency in future disease outbreaks, reassurances that their pronouncements won't be met with unscientific and stigmatizing repercussions will be needed.
Rwanda's swift response to Marburg is a testament to the country's growing health infrastructure and resilience. However, the real challenge ahead lies in managing regional vulnerabilities and balancing international expectations while working to effectively contain the outbreak at its source.