Neeraj Majhi, a 10-year-old from Odisha, one of India's poorest states, has been absent from school for two months. He often told his parents he felt too weak and fatigued to attend classes. Over time, Neeraj's father noticed a troubling pattern—his son seemed increasingly lethargic and uninterested in even simple activities at home. Concerned for his son's well-being, he took Neeraj to a local doctor. Blood test results confirmed that the boy was anemic.
Hundreds of miles away, in a small village in Bihar, India, Pooja Kumari, a bright and ambitious 14-year-old girl dreamed of becoming a teacher. In recent months, however, she was forced to skip school because of constant fatigue, headaches, and difficulty concentrating, leaving her teachers and parents worried. A visit to a health clinic revealed that Pooja was suffering from anemia, caused by poor nutrition and iron deficiency. The doctor prescribed iron supplements and advised the intake of iron-rich food.
Neeraj's and Pooja's stories highlight the prevalence of anemia among adolescents in India, underscoring the urgent need to address this health crisis and establish a causal link between anemia and school attendance. Anemia, characterized by the lack of healthy red blood cells or hemoglobin, limits the body's ability to carry oxygen. Its effects—fatigue, dizziness, and shortness of breath—may seem minor but have been suggested to have profound implications for everyday activities among adolescents as well, such as attending secondary school or doing homework.
The global prevalence of anemia is a significant public health challenge. A recent study estimated that anemia affects approximately 1.92 billion people worldwide, which equates to almost 25% of the global population. The World Health Organization (WHO) estimates that the anemia burden is disproportionately high among children and pregnant women, causing 50 million years of healthy life lost due to disability in 2019.
In India, iron-deficient anemia (IDA) is often referred to as a silent epidemic. Anemia is common in India given widespread nutritional deficiencies, particularly of iron, folic acid, and vitamin B12, caused by poor dietary habits and limited access to nutritious food. Additionally, factors such as frequent pregnancies, menstrual blood loss, infections, and lack of awareness about anemia exacerbate its prevalence, especially among women and children. Affecting more than half of adolescent girls and nearly one-third of boys, anemia could hinder school attendance by draining students' energy levels and cognitive abilities, researchers and policymakers have suggested.
A randomized controlled trial conducted in Delhi, India, for example, found that giving iron pills to preschool children—who were likely at risk of fatigue, reduced attention spans, and increased susceptibility to infections—boosted preschool attendance. Another study conducted in rural Peru found that supplemental iron pills given to adolescents reduced iron deficiency and led to significant improvement in cognitive functioning, test scores, and grade progression, including aspirations for anemic students.
A more recent randomized controlled trial conducted in Bihar found that though supplementing school lunches with double-fortified salt reduced the rate of anemia by 20% to 30%, it had few detectable impacts on cognitive development or test scores among grade 2 school children (age about 6 or 7). Similarly, a recent nationwide study using data on measured hemoglobin from India's National Family Health Surveys found mixed evidence, presenting new and unique insights into the relationship between anemia and school attendance.
India's current efforts to improve its education system are focused on increasing school retention, improving learning outcomes, and ensuring gender parity. Yet anemia remains a hidden barrier that may limit the potential of millions of adolescents and undermine the education system. With post-pandemic recovery and government programs including India's National Education Policy 2020 in full swing, addressing the condition seems more urgent than ever. Addressing anemia among adolescents could be crucial to driving educational success, reducing dropout rates, and ensuring gender equality.
The Anemia-Education Puzzle
India has one of the largest adolescent populations in the world—more than 250 million individuals between 10 and 19. Despite significant progress in primary school enrollment, secondary education remains a challenge. As of 2023, more than 40 million adolescents of upper secondary school age (14 to 18) were not attending school. Factors including socioeconomic barriers, opportunity costs of attending school for households and adolescents (such as doing laundry, cooking, and cleaning at home), and early marriage contribute to early school-leaving among adolescents. Poor health caused by anemia could be another.

Existing observational studies, however, typically do not account for all household-level factors, such as parental education, income, or psychological traits, which could confound the relationship between anemia and schooling. Furthermore, experimental studies can be expensive on a large scale and often limited to a specific school level, small regions, or subpopulations, leaving questions about its broader relevance for educational outcomes at other school levels or in other populations and settings. Similarly, little is known about potential differences in the relationship between having a certain severity of anemia (mild, moderate, severe, and life-threatening anemia) and schooling outcomes.
Study Findings
Using data on measured anemia from more than 250,000 adolescents surveyed between 2005 and 2021, the study investigated the relationship between anemia and school attendance among adolescents in India. Rather than comparing adolescents from different households, it compared the educational outcomes of adolescents living in the same household who had different levels of hemoglobin and anemia. This method allowed the researchers to isolate the relationship between anemia and school attendance by holding shared household characteristics constant. In addition to the household-level analyses (also known as household fixed-effects models), the study accounted for additional control variables, such as birth cohort, religion, household caste, and survey year (period) effects.
The findings offered a nuanced understanding of the relationship between anemia and school attendance in India. In more conventional analyses comparing adolescents across households, for example, adolescents with anemia were 2.5 percentage points less likely to attend school than their counterparts. However, when the educational outcomes of coresiding (living in the same household) adolescents were compared, no detectable relationship was observed between having any anemia and average school attendance. Although the health effects of anemia are well documented, its influence on school attendance appears to be more muted than previously thought. This suggests that other household and social factors play a more critical role in determining whether adolescents attend school.

The study also investigated the level of measured hemoglobin continuously (as opposed to simply having any anemia or not), differences in the relationship between the category of anemia severity and school attendance, and several other educational outcomes. The findings from those supplementary analyses suggest that although having any anemia may not directly hinder school attendance on average, having anemia, particularly higher levels of anemia severity (such as severe and life-threatening anemia) could affect human capital development due to disruptions in education. Those areas warrant further exploration.
Regional and Gender Variations
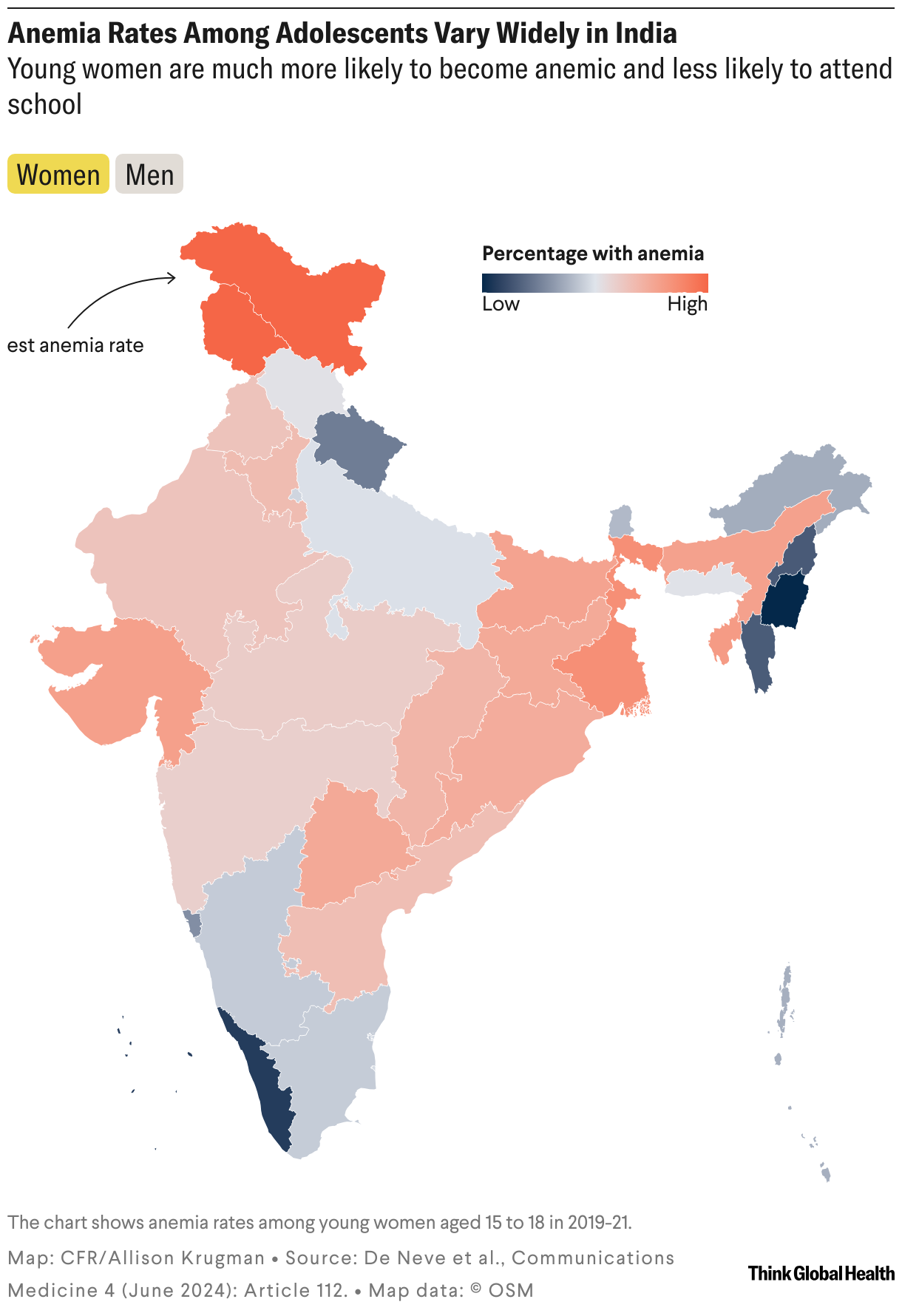
The study points to additional notable patterns. In particular, the proportion of adolescents in India with any anemia, as defined by the WHO, increased between the survey years 2005 and 2021. Specifically, the proportion of adolescents aged 15 to 18 with any anemia increased from 43.7% in 2005–06 to 55.7% in 2019–21. Girls were significantly more likely to be anemic than boys, more than half relative to approximately one-third of boys. Girls were also less likely to attend school, indicating broader gender disparities in health and education.
Regionally, the proportion of anemia and the school attendance rates among adolescents in the study sample varied widely. For example, anemia among adolescents ranged from 7.1% among young men in Lakshadweep to 78.8% among young women in Jammu, Kashmir, and Ladakh (Figure). Meanwhile, school attendance rates among adolescents ranged from 52.2% in Gujarat to 94.4% in Kerala. Those disparities highlight the importance of addressing regional and gender-specific challenges in health and education policies.
The proportion of adolescents aged 15 to 18 with any anemia increased from 43.7% in 2005–06 to 55.7% in 2019–21
Implications for Policy
The findings have implications for policymakers. If suffering from anemia has a limited detectable impact on average school attendance, focusing solely on reducing anemia as a strategy to improve educational outcomes may not yield considerable results. Approaches that target only adolescents at risk of anemia may not be enough to considerably improve school attendance at the population level in India. Instead, other interventions may be necessary to address the root causes, such as low perceived benefits of education among households and adolescents, financial costs associated with secondary school, opportunity costs of attending secondary school, and sociocultural factors.
That does not mean that anemia should be ignored. On the contrary, addressing anemia remains crucial to improving overall health and quality of life for adolescents. However, its role in enhancing educational outcomes may be less than previously assumed. Efforts to combat anemia should still be integrated with broader educational initiatives, such as providing school lunches fortified with iron and other micronutrients in schools or expanding school-based health education programs to raise awareness about the importance of nutrition and seeking health-care services to treat anemia.
As India works toward improving population health and achieving universal secondary education, studies like this offer information on where limited resources and efforts could be directed. Adolescence is a pivotal period of development when human capital investments can have large effects across the life course and for their communities. By addressing the broader structural barriers to education, India can ensure that every adolescent, regardless of health or socioeconomic status, has the opportunity to thrive.